

When a clinician assesses someone for autism, they're not just running through a simple checklist. They're using the official diagnostic criteria for Autism Spectrum Disorder (ASD) as a guide to understand a person's entire way of being.
These standards come from the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5), and they provide a framework for identifying a very specific combination of traits.
Understanding the Framework for Diagnosis
Think of the diagnostic criteria less like a rigid scorecard and more like a detailed blueprint. It helps a professional see how a person experiences and interacts with the world on a fundamental level.
This modern framework is a big deal. Before the DSM-5 was published in 2013, diagnoses like Asperger's Syndrome or Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS) were considered separate conditions. The current model unified them under the single umbrella of Autism Spectrum Disorder, recognizing that while autism looks different in everyone, the core characteristics are shared.
The Two Core Pillars of Diagnosis
For an autism diagnosis to be made, a person must show persistent challenges in two essential areas. It’s not one or the other; both must be present.
Here is a simple breakdown of these two core domains.
| Core Domain | Description of Deficits |
|---|---|
| A. Social Communication & Social Interaction | This involves ongoing difficulties with social back-and-forth, understanding nonverbal cues (like body language or tone of voice), and building or maintaining relationships. |
| B. Restricted, Repetitive Patterns of Behavior, Interests, or Activities | This can include repetitive movements, a strong need for sameness and routine, highly focused and intense interests, or sensory sensitivities (being over- or under-sensitive to sound, light, or touch). |
These two pillars form the foundation of the entire diagnostic process.
Ultimately, the goal is to see the world from the individual's perspective. The process asks: How does this person's unique neurotype shape their social understanding and their behavior? This ensures a diagnosis is more than a label—it's a key to unlocking the right support.
It's also crucial to understand that these characteristics must have been present in early childhood. Sometimes they don't become fully obvious until a person is older and social demands exceed their capacity. Most importantly, these traits must cause significant, real-world challenges in a person's life, whether at school, at work, or in their relationships.
The Evolution of Diagnosing Autism
To really get a handle on today's diagnostic criteria for Autism Spectrum Disorder (ASD), it’s helpful to take a look back. The way clinicians identify autism has been on quite a journey—it’s a story of major shifts driven by decades of research and a growing, more compassionate understanding of human neurodiversity.
In the beginning, the whole idea of autism was murky, often tangled up with other conditions. It took years of work for it to stand on its own as a distinct neurodevelopmental profile. This long road is precisely why today’s standards are so carefully designed to offer a nuanced, holistic view of each person.
From Childhood Schizophrenia to A Distinct Diagnosis
The diagnostic landscape for autism has changed dramatically since the term first popped up in the Diagnostic and Statistical Manual of Mental Disorders (DSM). Initially, in the DSM-I (1952), autism was barely a footnote, mistakenly lumped in with schizophrenic reactions in children. It was a long wait until the DSM-III in 1980 before "Infantile Autism" was finally recognized as its own separate diagnosis.
This was a landmark moment. For the first time, specific criteria were laid out, including an onset before 30 months of age and noticeable differences in language development.
Even with this step forward, the early definition was pretty rigid. Imagine trying to describe a sprawling, vibrant rainforest using only a few basic color swatches—you’d miss all the texture and variety. The picture was incomplete. As researchers learned more, it became clear that a much broader, more flexible framework was essential to truly capture the autistic experience.
The core concept began to shift. We moved away from trying to pinpoint a single, narrow "disorder" and toward recognizing a wide spectrum of neurological differences. This change finally acknowledged that autism shows up differently in every single person, shaped by their unique strengths, challenges, and personality.
The Move Toward a Unified Spectrum
The real game-changer arrived with the DSM-5 in 2013. Before this update, the diagnostic manual had several separate-but-related conditions under the Pervasive Developmental Disorders umbrella, including:
- Autistic Disorder: What most people thought of as "classic" autism.
- Asperger's Disorder: Marked by social challenges but without significant delays in language or cognitive skills.
- Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS): A catch-all diagnosis for people who had some, but not all, of the traits of the other two.
This piecemeal approach often led to confusion. The lines between the diagnoses were blurry, making things difficult for families and clinicians alike. The DSM-5 swept this away by combining these labels into one single diagnosis: Autism Spectrum Disorder (ASD).
This was far more than a simple name change; it was a fundamental shift in thinking. It was an official recognition that these conditions were all points on the same continuum, differing by the degree and combination of traits, not by type. This unified approach gives us a much more accurate and helpful way to understand an individual's specific support needs without getting bogged down in overlapping labels.
For a closer look at what this means for individuals today, you can read our detailed guide on the autism diagnosis process explained. Understanding this history is vital—it’s the foundation upon which today's comprehensive and flexible diagnostic criteria are built.
Breaking Down the DSM-5 ASD Criteria
When clinicians evaluate for autism, their primary guide is the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5). Think of it less like a rigid checklist and more like a detailed map of the brain's landscape. It helps a professional identify the specific combination of traits that point to an Autism Spectrum Disorder (ASD) diagnosis.
The biggest shake-up in recent memory happened in 2013 when the DSM-5 was released. This update moved away from separate labels like Asperger's Disorder and Autistic Disorder, unifying them under the single umbrella of ASD. It also softened the strict "onset before age 3" rule, recognizing that symptoms simply need to appear in the "early developmental period." This was a huge step, allowing for diagnosis based on current behaviors or what someone remembers from childhood. You can read more about this landmark shift and what it meant for the community.
This modern approach boils it down to two core areas. For a diagnosis to be made, a person has to show persistent, meaningful differences in both of them.
Criterion A: Social Communication and Social Interaction
The first pillar of an ASD diagnosis involves ongoing differences in how a person connects and communicates with others. This goes much deeper than just being shy or introverted; it's about fundamental differences in the brain's wiring for social give-and-take.
The DSM-5 requires that all three of the following challenges are present:
-
Deficits in Social-Emotional Reciprocity: This is the natural back-and-forth of a social exchange. In practice, this might look like someone struggling to start or maintain a conversation, seeming disinterested in small talk, or enthusiastically sharing about a passion without picking up on cues that the other person isn't following along.
-
Deficits in Nonverbal Communicative Behaviors: This is all about the unspoken language we use every day. An individual might not use typical eye contact, might have a limited range of facial expressions, or could have a tough time reading body language, gestures, or tone of voice in others.
-
Deficits in Developing, Maintaining, and Understanding Relationships: This gets at the messy, complex business of making and keeping friends. It can show up as difficulty making friends in the first place, a strong preference for being alone, or trouble adjusting one's behavior for different social settings, like a classroom versus a playground.
It's so important to get the framing right here. From a neurodiversity-affirming viewpoint, these aren't character flaws or failures. They are simply differences. An autistic brain is wired to communicate and relate differently—often in a more direct, logical way—than a neurotypical brain.
This image really helps to visualize how the two main diagnostic pillars work together.
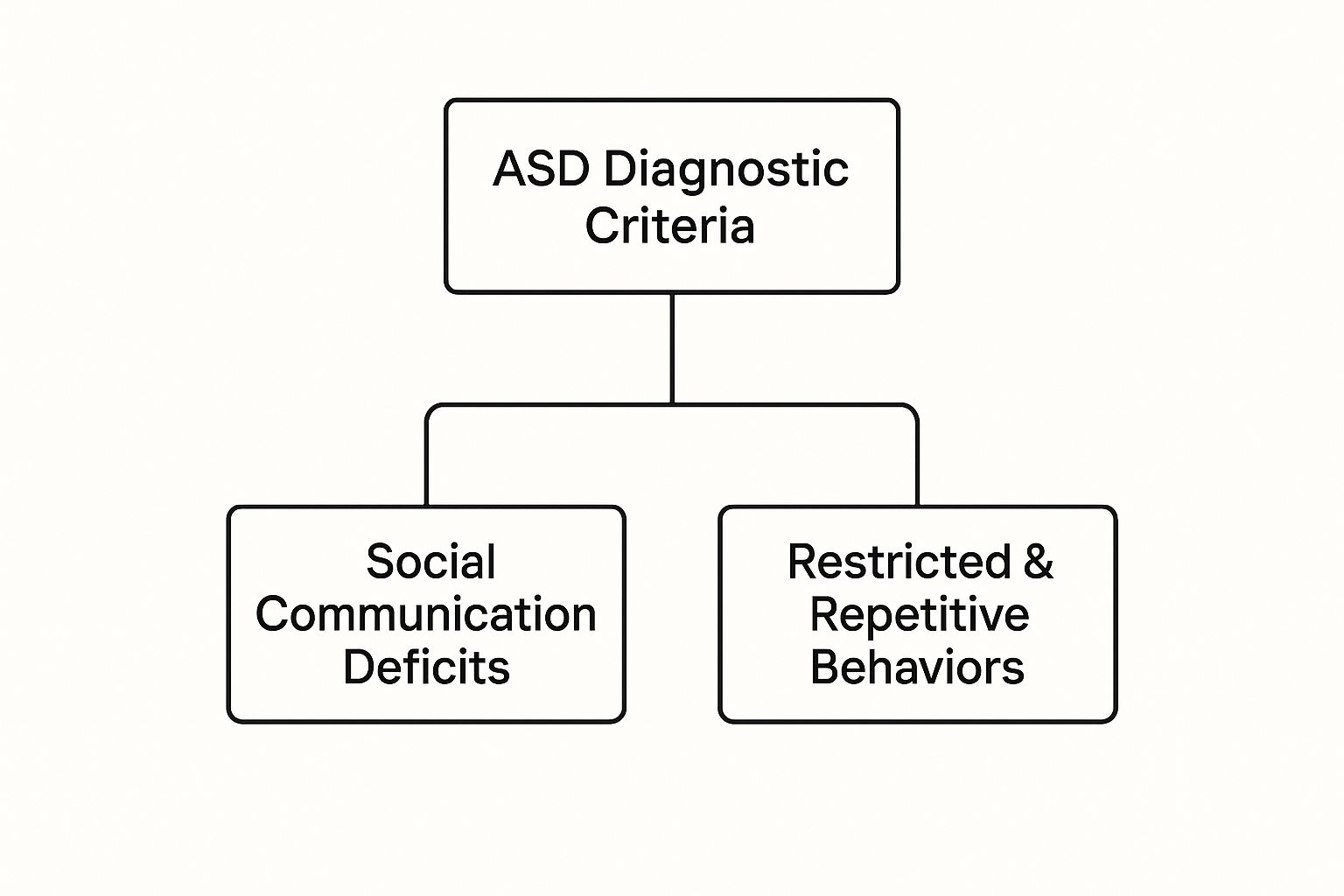
As you can see, a diagnosis requires solid evidence from both of these distinct, yet interconnected, domains.
Criterion B: Restricted and Repetitive Behaviors
The second pillar focuses on a pattern of restricted interests and repetitive behaviors. To meet this part of the criteria, a person has to show at least two of the following four patterns.
-
Stereotyped or Repetitive Motor Movements, Use of Objects, or Speech: This is what many people think of as "stimming"—behaviors like hand-flapping, rocking, or finger-flicking. It can also include lining up toys with precision or repeating words and phrases (echolalia).
-
Insistence on Sameness and Inflexible Adherence to Routines: Predictability is a safe harbor for many autistic people. This can manifest as extreme distress over small changes, needing to eat the same foods every day, or insisting on taking the exact same route to school. Routines are a powerful tool for managing a world that often feels chaotic.
-
Highly Restricted, Fixated Interests that are Abnormal in Intensity or Focus: We often call these "special interests." An autistic person might develop an incredibly deep, passionate, and encyclopedic knowledge of a specific topic, whether it's train schedules, dinosaurs, or a particular video game.
-
Hyper- or Hypo-reactivity to Sensory Input: This involves being either over-sensitive (hyper) or under-sensitive (hypo) to the world around them. One person might be completely overwhelmed by bright lights and loud sounds, while another may not seem to notice pain or extreme temperatures. It can also include a deep fascination with certain sensory experiences, like smelling objects or feeling specific textures.
The Other Essential Pieces
Just meeting the criteria for A and B isn't quite enough. The DSM-5 wisely includes three final checks to ensure the diagnosis is accurate and helpful.
Criterion C: The symptoms have to be present from early childhood. The key here is that they might not have become a real problem until social situations got more complicated, or they may have been masked by coping strategies the person learned over the years.
Criterion D: The symptoms must cause "clinically significant impairment." This is a crucial point. The traits must create genuine, real-world challenges in social, school, or work life. It isn't a diagnosis for a quirky personality; it's for when these differences impact daily functioning.
Criterion E: The challenges aren't better explained by an intellectual disability or a global developmental delay. While autism can certainly co-occur with an intellectual disability, the social communication difficulties must go beyond what would be expected for that person's overall developmental level.
How Severity Levels Shape an ASD Diagnosis

Getting an Autism Spectrum Disorder diagnosis isn't just a simple "yes" or "no." The way we approach ASD diagnostic criteria today is far more nuanced, creating a detailed profile of an individual by using specifiers. The most significant of these are the severity levels, which tell us about a person’s support needs.
Think of it this way: the diagnosis confirms someone is on the spectrum, but the severity levels describe the terrain of their unique journey. This shift is critical. It moves the conversation away from a mere label and toward a practical understanding of what kind of support will help that person truly thrive. These levels aren't a judgment of someone's potential or worth; they're a clinical tool for mapping out effective, personalized care.
The Three Levels of Support
The DSM-5 lays out three distinct severity levels. A clinician assigns a level for both of the core symptom domains—one for Social Communication and another for Restricted, Repetitive Behaviors. This is a key point. It means someone might be a Level 2 for social communication challenges but a Level 1 for their repetitive behaviors. Any combination is possible.
This dual-level system acknowledges that a person’s need for support can look very different across various parts of their life. Let’s break down what each level actually means in the real world.
Level 1: Requiring Support
This is often what people are thinking of when they use outdated terms like "high-functioning autism." Someone at Level 1 has clear challenges in social situations. They might find it tough to start a conversation, or their interest in social interaction might seem reduced. Without support, their efforts to build friendships can often fall flat.
When it comes to repetitive behaviors, a person at this level might have such a strong need for routine that it gets in the way of adapting to change. For example, they might find switching from one task to another extremely difficult or struggle with planning and organization.
Level 2: Requiring Substantial Support
At this level, social difficulties are much more obvious, even when support systems are in place. The person may have very limited interest in social contact, use unusually brief sentences, or speak in a very direct manner. Their nonverbal communication—things like eye contact and body language—is noticeably different from that of their peers.
Repetitive behaviors at Level 2 are frequent enough to be apparent to a casual observer and interfere with daily functioning in many situations. Distress over a change in routine is more intense, and it's much harder for them to shift their focus away from a particular interest.
Level 3: Requiring Very Substantial Support
Individuals at Level 3 face severe challenges with both verbal and nonverbal social communication, which significantly impacts their day-to-day life. They may have very few intelligible words and rarely initiate social interaction. When they do, it's often to meet immediate needs and nothing more.
At this level, repetitive behaviors are extreme and markedly interfere with their ability to function. The person has great difficulty coping with change and can show intense distress when a routine is broken. Their restricted interests or repetitive actions can make it incredibly difficult to participate in most activities.
It's vital to remember these levels are about the amount of support needed, not the individual's inherent abilities. The goal is to match the support to the need, ensuring that every autistic person has the resources to lead a happy, healthy, and fulfilling life.
Beyond the Levels: Additional Specifiers
A truly comprehensive diagnosis doesn't stop with the levels. Other specifiers add even more clarity, painting a complete and actionable picture.
A clinician will also specify:
- With or without accompanying intellectual impairment: This notes whether the person’s intellectual development is on a typical path or if they also have an intellectual disability.
- With or without accompanying language impairment: This clarifies if there are language delays or differences beyond what's expected from their social communication challenges alone.
- Associated with a known medical or genetic condition or environmental factor: This is used when the autism is connected to a condition like Rett syndrome or Fragile X syndrome, or if there was exposure to a substance like valproate during pregnancy.
Put together, the severity levels and these additional specifiers transform the general ASD diagnostic criteria from a clinical checklist into a practical roadmap for support.
Navigating the Comprehensive ASD Assessment Process

Getting an accurate Autism Spectrum Disorder (ASD) diagnosis isn't like a quick lab test that gives a simple positive or negative result. It's much more like putting together a detailed puzzle. A definitive conclusion rarely comes from a single appointment or one professional’s opinion. Instead, it’s a careful, collaborative journey that draws on multiple sources of information to paint a clear and complete picture.
This entire process is typically guided by a multidisciplinary team—a group of specialists who each look at the individual through a unique professional lens. This teamwork ensures that every aspect of a person’s development, behavior, and experience is thoughtfully considered.
Assembling the Diagnostic Team
A truly comprehensive evaluation brings together experts from different fields, with each one contributing a vital piece to the puzzle. While the exact makeup of the team can vary based on individual needs and available resources, it often includes:
- Developmental Pediatricians: They examine the child’s overall physical health and developmental milestones.
- Child Psychologists or Neuropsychologists: These experts assess cognitive abilities, behavior, and emotional well-being.
- Speech-Language Pathologists: Their focus is on communication skills—everything from spoken words to nonverbal cues.
- Occupational Therapists: They evaluate sensory processing, fine and gross motor skills, and the ability to perform daily living activities.
This team-based approach is absolutely essential. It helps clinicians distinguish autism from other conditions that might have overlapping traits and provides a full understanding of an individual's unique profile of strengths and challenges.
The guiding principle is simple: see the whole person. By weaving together insights from developmental history, direct behavioral observation, and formal testing, the team can confidently determine if the ASD diagnostic criteria are met. Just as importantly, this holistic view allows them to create a support plan that is genuinely personalized.
The broadened criteria in the DSM-5, along with a huge increase in public awareness, have meant that more people are being identified. For example, recent studies in the United States show an ASD prevalence of about 1 in 36 children. This shift underscores just how critical thorough, team-based assessments are for ensuring every diagnosis is both accurate and meaningful.
The Gold-Standard Assessment Tools
To gather objective information, clinicians rely on standardized, research-backed tools. These aren't pass-fail tests. Think of them as structured ways to observe and measure behaviors that are directly relevant to autism. Two of the most respected and widely used tools in the field are the ADOS-2 and the ADI-R.
1. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2)
This is a semi-structured, play-based assessment. A trained clinician guides the individual through a series of social activities specifically designed to create natural opportunities for communication, social interaction, and imaginative play. The clinician carefully observes and scores the person's responses in real-time. For a toddler, this might look like playing with bubbles or a toy tea set. For an adult, it could involve a conversation about friendships or work.
2. Autism Diagnostic Interview-Revised (ADI-R)
This tool is a detailed, structured interview conducted with parents or primary caregivers. It's designed to gather a deep and thorough history of the person's early development and current behaviors, focusing specifically on the core symptom areas of ASD. The ADI-R is crucial because it provides that vital historical context that a one-time observation like the ADOS-2 simply can't capture.
When used together, these tools—combined with the clinical team's expert judgment and valuable input from family and teachers—form the bedrock of a reliable diagnosis. Finding a qualified team to perform this evaluation is a critical first step. If you're looking for guidance, our article on finding autism evaluation and diagnosis services in Minnesota is a great place to start.
Answering Common Questions About Getting an ASD Diagnosis
Even after getting familiar with the ASD diagnostic criteria, it's natural to have more questions. The journey to an assessment can feel overwhelming, so let's tackle some of the most frequent concerns head-on with clear, practical answers.
Getting straight on these points can make a world of difference. You’ll feel more prepared and confident, whether you're exploring a diagnosis for yourself, your child, or just want to understand the process better. My goal here is to cut through the complexity and give you information you can actually use.
Can Adults Really Get a Proper Diagnosis?
Yes, absolutely. It's becoming more and more common for adults to be diagnosed with autism for the first time. Even though autism is a developmental condition with roots in early childhood, many people learn to "mask" or camouflage their traits, sometimes for their entire lives.
Often, it’s a major life change—like a new job, a relationship ending, or becoming a parent—that makes the old coping strategies fall short, leading someone to finally seek answers.
A thorough adult assessment is a deep dive. It’s not just a quick checklist. A good clinician will look at:
- Your entire life story: They'll want to hear about your childhood, how you made friends (or didn't), your school experiences, and how you navigated social situations over the years.
- Your life right now: The evaluation will focus on how your traits affect your job, relationships, and day-to-day functioning today.
- Direct interaction: Tools like the ADOS-2 can be adapted for adults, giving the clinician a chance to see your social and communication style in a structured, but not scary, setting.
The whole process is designed to be comprehensive and affirming. For many adults, it’s the moment they finally receive a name for a lifetime of feeling different, and that validation can be incredibly powerful.
What Happens If I Don't Agree with the Result?
This is a totally valid concern. If you get an assessment outcome that just doesn't sit right with you, you have every right to question it. Your first move should be to schedule a detailed feedback session with the clinician. Ask them to walk you through exactly how they reached their conclusion and what data they used.
If you're still not convinced, getting a second opinion is a perfectly reasonable next step. Find another qualified professional or, even better, a multidisciplinary team. Experience levels among clinicians can vary, especially when it comes to diagnosing autism in women, adults, or anyone whose traits don't fit the classic mold. A fresh set of eyes can make all the difference.
Remember, a diagnosis is supposed to be a helpful tool. Its purpose is to unlock understanding and support, not to put you in a box. You are your own best advocate, so keep seeking clarity until you have an answer you can trust.
It's also important to know that many autistic people have other medical conditions that can overlap or co-occur. Looking into these can sometimes bring more clarity. For a deeper dive on this topic, check out our guide on understanding autism and its associated medical conditions.
Article created using Outrank


